
The Book of Numbers
The Book of Numbers
Informed Consent and the Genomic Vaccines

Risky Business
There is an elephant in the vaccination room. It’s a bedrock ethic within the medical establishment and scientific research facilities around the world and it’s called Informed Consent. That elephant came to the fore when the first vaccine in the US was granted Emergency Use Authorization (EUA) and the medical establishment and it’s partners in public health along with the corporate media demanded a “Moon Shot” vaccination campaign on the heels of President Trump’s Operation Warp Speed. That ethic has its roots in not only the Hippocratic Oath of “Do no harm” but also in the Nuremberg Code No 1: “The voluntary consent of the human subject is absolutely essential.”
“This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonably to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment.
The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.”
The voluntary part involves the patient or study participant being informed of the risks as well as the benefits and all medical professionals are supposedly trained to understand and follow that code. The Nuremberg Code is not an abstract ethical detour meant to delay the men/women of action during an emergency but a bedrock principle developed in the aftermath of Nazi Germany’s horrific pursuit of “the Science” using human beings as disposable test subjects in their Eugenics program. The Nuremberg Code is directly involved in discussions about promoting dubious and untested genomic therapies at Warp Speed on a global basis with little regard to flashing red warnings and the informed consent of the global trial participants in an extended roll-out of the Phase III trial during this pandemic. Whether you’ve taken the vaccines or not, you are part of that trial. Many intend on being in the control group.
Central to informed consent is the risk/benefit calculation. That is where the life insurance company example comes into the discussion. No doubt if an insurance adjuster were to weigh in on how to insure and individual against the prospect of a COVID-19 infection, she’d make a cold calculus on the risk profile of that individual. A profit driven one but an accurate one to prevent loss to her employer. Here’s what it looks like for the risk profiles of a serious COVID-19 illness and death based on age before the vaccination roll-out from Forbes using CDC data:


“Even for children who actually are infected with the coronavirus, the risk of dying is extraordinarily low. Covid-19 patients under age 20 are 17 times as likely to die due to other causes of death this year than they are to become Covid-19 fatalities. A different way of looking at this risk is that 30 micromorts is equivalent to the fatality risk of driving a car 7,500 miles. The average male driver covers this distance in less than a half a year (female drivers take about 9 months to cover the same distance). There are 210 million licensed drivers. In short, there are tens of millions of Americans who voluntarily expose themselves to that level of risk without giving it a second thought.
In contrast 54,000 micromorts is roughly 1.5 times as high as the risk of dying while climbing Mt. Everest. Few Americans would voluntarily undertake any activity for which the risk of dying exceeded five percent. The average person age 70 or greater already faces nearly a four percent risk of death from other causes. Getting infected with Covid-19 multiplies this baseline fatality risk by 140 percent! In contrast, someone under 20 years old who gets Covid only increases their baseline risk of death by six percent.” - Forbes
Here’s the most current risk-of-death picture for age in the U.K. for the Delta variant that just finished its surge:

Here’s what I found over at the CDC on risk-of-death compared to the chart above:

That’s a current 2021 snapshot of the US “rate ratios” with a reference group that more or less tells you nothing other than orders of magnitude not the actual risks-of-death in a population. But back to the first Forbes chart. They use micromorts (deaths per million) AND they compare the COVID deaths to ALL deaths for that demographic. For instance, if you are between 20-49 years your risk of a COVID illness ending in death is .0002 compared to any kind of death at .001686 in a years term. Your chances just went up by two ten-thousandths of one certain death of a COVID illness for 2020. Follow? And that’s only if you’re infected with SARSCov2 per the chart’s note. The percentage now of how much of the US population contracted an infection is 10.6% according to the CDC (35Mn/330Mn). But even the CDC admits that’s a gross under-count. Many Americans have been infected but never developed a symptomatic illness worth testing for or were asymptomatic altogether. That means the chart’s denominator for population infected is much higher and the death ratio that much smaller whatever the real number of infections total per million are.
At this point in late 2021, the complicated differentials you need to calculate to project forward on what the real risk of infection and death are going forward is just too much even for the CDC apparently. But you can infer a lot from the past 18 or so months on your own demographic and other risk profiles. You can also make a good bet that at least half of the US population is now somewhat naturally immune via previous infections I noted above (not the oasis/mirage of herd immunity still being offered as a reason to mass vaccinate). But all bets are off if a super variant develops immune escape because of the very vaccines the US is mass dosing its population with.
Manufactured Consent
When a new therapy, drug or vaccine is up for approval at the FDA it demands that the medical profession, hospitals and doctors who prescribe that new regimen are up to snuff on the ethic of Informed Consent with their patients. This includes participants in any study involving that regimen.
This goes directly back to the Hippocratic Oath and the Nuremberg Code. It is medical ethics 101 but it’s also glossed over all too often at the point of follow-up by the FDA and inside the doctor’s office. But it comes into sharp focus during the episode we are living through – the roll-out of a novel therapy the drug companies refer to as vaccines for EUA approval during this pandemic that are meant for the arms of hundreds of millions if not billions on the planet. A basic piece of that information forming that consent is the benefit/risk calculation.
When Pfizer went for its EUA (later Moderna) they had their publicity sheets ready to go for the corporate media when on November 9, 2020 it announced a 90% efficacy vaccine BNT162b2 (no details on what that “efficacy” related to) just that it was an incredibly effective vaccine. It already had a $2 billion contract with the Federal Gov’t and the stock price jumped 23% in early trading. It was a modern day miracle and the global media toasted Pfizer and its partner in Germany, BioNTech, for bestowing upon humanity this “light at the end of the tunnel” (just one of the many superlatives from the World Economic Forum announcement). The biotech industry wheels were set in motion not to be impeded by any nay-saying from the Operation Warp Speed skeptics or molecular scientists who might dissent. And it was safe. Presumably. We needed it to be safe.
95% Solution
That 90% soon became 95% and we got pummeled with that one statistic for weeks on end. There was very little media reporting about the endpoints of the Phase III trials they ran for two months on participants to get the results. You could find the abstract and some trial data online but it was a full out blitz to sell this as the cure to COVID-19 and snuff out the pandemic by all major media outlets and on Silicon Valley social media.
“To save time, the companies began manufacturing the vaccine before they knew whether it would be effective. They now expect to produce up to 50 million doses, or enough to protect 25 million people this year.” - World Economic Forum
That 95% is key to understanding what happened to Informed Consent and how we got to this point where we are faced with the fading efficacy of the vaccines, an expanding set of incoming data at the VAERS (Vaccine Adverse Effects Reporting System) website with their alarmingly high incident reports and the vaccine’s long term unknown impacts upon the human body.1
Pfizer, later Moderna and the others following their lead knew that to sell these novel mRNA vaccines they’d have to play up the 95% solution. To help this along they’d have to skew the benefit/risk calculation of true Informed Consent that the medical establishment is expected to follow through in practice. Conflicts-of-interest within the watchdogs at the NIH – Dr Fauci being top dog – greased the skids to get the research community inside the NIH to stay silent during the campaign. Almost (see below).
Absolutes
It must be made clear the difference between the risks of contracting a COVID infection in the first place as opposed to the risks of known and unknown adverse effects of receiving the therapeutic though both come into play with Informed Consent. Once that distinction is clear you can seperate and simplify the risk/benefit calculation for any personal profile and make an informed decision on whether to take the therapeutic or not. To do that a doctor, researcher, hospital administrator or media personality hired to sell the products to the public has a responsibility to introduce the two relevant calculations that are embedded in the Phase III drug trials: Relative Risk Reduction and Absolute Risk. Conveniently for the pharmaceutical companies, the FDA waved off on that piece of Informed Consent in the EUA by approving Pfizer’s fact sheet to recipients and caregivers. The sheet never mentions the Absolute Risk Reduction for the experimental product inside its own Phase III trials as stark and clear that information is. That meant that doctors and the compromised medical establishment including the CDC could on the one hand trumpet the 95% (Real Relative Risk Reduction) and on the other ignore Absolute Risk Reduction with caregivers and patients in consenting to vaccination. That is a direct violation of Informed Consent and the FDA knows it because it violates this all the time in approving drugs, therapeutics and interventions. Only this time it involves expanding clinical trials globally through an EUA of a new technology never approved before without any track record. This wasn’t hidden or lost by some at the NIH itself either. On its PubMed.gov website Ronald B. Brown posted an analysis of the Phase III trials with a short take entitled Outcome Reporting Bias in COVID-19 mRNA Vaccine Clinical Trials and a conclusion pointing out that the Absolute Risk reduction calculation is essential in avoiding a phenomenon known as reporting bias which is critically related to Informed Consent and geting good data signal in general as to the results and impacts upon a global population from the vaccines. Playing up the ‘slam dunk’ could set up the global experiment for highly skewed and biased reports confirming the slam dunk. No apologies to George Tenet.
Absolute Risk Reduction calculation is central also to a physician/patient decision on electing for a therapeutic, drug, intervention even if it’s just a fact sheet quickly handed over in a 5 minute consultation. If the chances of contracting Dengue Fever in the Upper Peninsula of Michigan is near zero you might not want to take that risky vaccine for it and you’d expect your doctor to inform you of that vital piece of information. And that is all that Absolute Risk reduction is about compared to RRR and that 95%. This calculation is not that complicated either with the data of the Phase III trials. The math is further down this piece but it’s simple division then subtraction in ratios based on the same data used to get the 95% Solution of who got a symptomatic case or above of COVID-19 in both the vaccinated group and the control (placebo) group. Everyone that does “the Science” knows this, at least deep within the bowels of research institutes as the above article at PubMed shows. The medical establishment and hospitals stopped insisting that doctors understand this since most practitioners aren’t trained in research. We’ve seen the FDA overlook their own requirements for EUA fact sheets of the mRNA and adenovector virus vaccines and the local public health authorities, well they never had a clue to begin with since they’re basically bureaucrats. From the FDA.gov website on fact sheets:
How will vaccine recipients be informed about the benefits and risks of any vaccine that receives an EUA?
FDA must ensure that recipients of the vaccine under an EUA are informed, to the extent practicable given the applicable circumstances, that FDA has authorized the emergency use of the vaccine, of the known and potential benefits and risks, the extent to which such benefits and risks are unknown, that they have the option to accept or refuse the vaccine, and of any available alternatives to the product. Typically, this information is communicated in a patient “fact sheet.” The FDA posts these fact sheets on our website.
Yet the FDA cares less about informing Americans of a basic risk ratio percentage available from the Phase III trials that gives a completely different context to the benefits of taking the vaccines.
So we’ve found ourselves with a health system, public health authorities and a medical establishment primed to ignore Informed Consent on the first ever global medical experiment during a pandemic involving genomic substances passing as vaccines. The “do no harm” thing weighed against the real world risks of a COVID-19 infection for any particular person who ultimately should have final say over their personal health through free and informed choice per the Nuremberg Code.
Do The Math
I found this at Orthodox Reflections of all places since they did the most cogent walk through analysis. I recommend you go there and read the whole piece:
“Why are ARR and RRR very important? Very simply, let’s assume you have 100 people in a Treatment group and another 100 people in a Control or placebo group. Then, let’s say that 2 people get Disease X in the Control group while one person gets Disease X in the Treatment group. The Relative Risk Reduction or RRR in this example is 50% because one diseased person is 50% or half of 2 diseased people. However, the Absolute Risk Reduction (ARR) is only 1% because in the treatment group, only one fewer people out of 100 participants got Disease X. You can also work it out using these formulas:
In the Treatment group, 1/100 got Disease X = 1% which is the EER (Experimental Event Rate)
In the Control or placebo group, 2/100 got Disease X = 2% which is the CER (Control Event Rate)
Absolute Risk Reduction (ARR) = CER – EER = 2% – 1% = 1%
In a subtraction the % signs carry through the equation and are kept.
4. RRR (Relative Risk Reduction) = ARR divided by CER = 1% divided by 2% = ½
In a division, the % signs cancel each other out and are not kept, but ½ is the same as 50%.
Let’s say the Treatment in this example had side effects, as most treatments do. If a patient were offered this Treatment and was told that the “efficacy” (how well the treatment works) was only 1% (the ARR) which is the true efficacy, this patient would be much less likely to accept the Treatment and its side effects than if he or she were told the efficacy was 50%. Fifty percent sounds a lot more promising than 1% but it reflects only the comparison between the diseased people of each group. The ARR or 1% efficacy is much more accurate as it reflects how many more people out of 100 will be protected from Disease X as a result of the Treatment. To just say that the Treatment is 50% effective in this scenario by ignoring the ARR is to introduce outcome reporting bias.” (see Ronald Brown at PubMed.gov above)
Now let’s apply the Pfizer BNT162b2 Phase III endpoint results. From Orthodox Reflections continued:
Analysis of Pfizer’s Data
In the vaccine group, 8/18,198 got Covid-19 infection (not death) = 0.044% This is the EER (Experimental Event Rate)
In the Control (placebo) group, 162/18,325 got Covid-19 infection (not death) = 0.884%
This is the CER (Control Event Rate)
ARR (Absolute Risk Reduction) = CER – EER = 0.884% – 0.044% = 0.84% = 0.84/100 = 0.0084
RRR (Relative Risk Reduction) = ARR divided by CER or 0.84% divided by 0.884% = 0.95
As this formula involves division, the percentage signs cancel out. 0.95 is the same as which is what the Pfizer study reports for “efficacy.” An “efficacy” of 95% gives the impression that one is 95% less likely to catch Covid-19 if one is vaccinated with Pfizer’s Covid-19 vaccine. However,
ARR or Absolute Risk Reduction, which is 0.0084 or 0.84%, is actually less than 1%
As shown under the ARR and RRR heading above, the ARR (of any study) is far more accurate than the RRR, but clearly, 95% sounds much more compelling than <1%. Referring to the “efficacy” of the Pfizer vaccine as 95% is not technically incorrect, but it is very misleading as this value does not properly inform the vaccine recipient. Such misrepresentation is at the very least unethical and at most illegal in many countries which require informed consent. Unfortunately, it is easy for outcome reporting bias to escape detection since the average individual, including the average doctor, does not understand ARR and RRR and will automatically assume that “95% efficacy” means 95% less likely to get Covid-19 in the real world.
Another way of understanding the ARR is by calculating the number needed to treat, or the NNT. The NNT in this case would be the number of people who would need to be vaccinated to prevent ONE case of Covid-19 infection (not death, since the study did not measure death) Here is the calculation:
NNT = 1/ARR = 1 divided by 0.84% = 1/0.0084 = 119 people.”
What NNT or more specifically Number Needed to Vaccinate in this case (NNV) directly implies through Absolute Risk Reduction is that for every one infection you prevent (no matter how moderately symptomatic – maybe just a PCR test and a headache per Pfizer’s methodology) you would have to vaccinate 119 people who would get no benefit from vaccination because the numbers only imply it works 1/119 of the time compared to the control group who got no vaccine. Follow?
Here’s Ron Brown’s numbers at Pubmed.gov back in February of 2021:
Abstract
Relative risk reduction and absolute risk reduction measures in the evaluation of clinical trial data are poorly understood by health professionals and the public. The absence of reported absolute risk reduction in COVID-19 vaccine clinical trials can lead to outcome reporting bias that affects the interpretation of vaccine efficacy. The present article uses clinical epidemiologic tools to critically appraise reports of efficacy in Pfzier/BioNTech and Moderna COVID-19 mRNA vaccine clinical trials. Based on data reported by the manufacturer for Pfzier/BioNTech vaccine BNT162b2, this critical appraisal shows: relative risk reduction, 95.1%; 95% CI, 90.0% to 97.6%; p = 0.016; absolute risk reduction, 0.7%; 95% CI, 0.59% to 0.83%; p < 0.000. For the Moderna vaccine mRNA-1273, the appraisal shows: relative risk reduction, 94.1%; 95% CI, 89.1% to 96.8%; p = 0.004; absolute risk reduction, 1.1%; 95% CI, 0.97% to 1.32%; p < 0.000. Unreported absolute risk reduction measures of 0.7% and 1.1% for the Pfzier/BioNTech and Moderna vaccines (emphasis mine), respectively, are very much lower than the reported relative risk reduction measures. Reporting absolute risk reduction measures is essential to prevent outcome reporting bias in evaluation of COVID-19 vaccine efficacy.
Slight difference between Orthodox Reflections .84% and Ron Brown’s .7% but that’s just a variation on the total number of participants the two examples plugged in. The point is it’s <1%.
And that’s it. It’s a lot different to claim your therapeutic intervention has a 95% “efficacy” than that it reduces your risk of infection by less than 1% to repeat Orthodox Reflections. A world of difference.
Remember too that the RRR vs ARR calculations apply to all demographics in aggregate – at least the ones included as participants in the trials. Some groups like pregnant women (which in the original write up in the New England Journal of Medicine (NEJM) never mentioned at all – Pfizer has announced in February they’re doing one now with 4,000 participants), the immune compromised, anyone with a history of a COVID-19 infection among other risky trial participants that might nix the 95% score, were not included.
But still, the trial’s data includes nominally every demographic and that that slim <1% ARR is even slimmer based on how much younger you are from the 52 years old median age of the trial. Much smaller. Plus, you absolutely have to weigh the adverse effects of the vaccines themselves, a bunch we have no idea will manifest in the long term against those very tiny odds if you are young.
Outcomes
This risk breakdown based on Pfizer’s own ballyhooed results was done back earlier this year but the same math applies today with the Delta variant and the others surely to follow if and when the pharmaceutical companies release that data on the “efficacy” of their concoctions on those. Here’s a current chart put on the same PubMed.gov that was posted cryptically as “COVID-19 vaccine efficacy and effectiveness-the elephant (not) in the room” with both RRR and the NNV (number needed to vaccinate) for all the vaccines as of July 2, 2021 by Piero Olliaro, Els Torreele and Michel Vaillant:
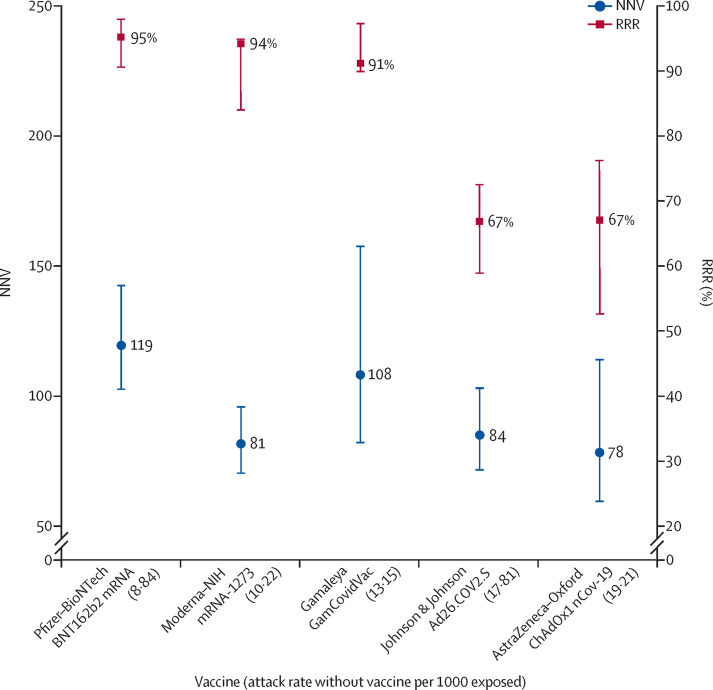
[RRR and NNV with 95% CI ranked by attack rate in the unvaccinated (placebo) group for five COVID-19 vaccines The lower the NNV and the higher the RRR, the better the vaccine efficacy. RRR=relative risk reduction. NNV=numbers needed to vaccinate. NIH=US National Institutes of Health]
Clearly the Moderna vaccine wins out over Pfizer’s by this chart’s metrics. There must be a feud brewing inside the NIH and these cryptic postings at each other on PubMed.gov must be the outlet. Again, the NNV is an inverse expression of the Absolute Risk Reduction percentage quantifying it in persons needed to vaccinate to get one person protected from only an infection however symptomatic (not death since it was never an endpoint in the trials). The rest get nothing but the vaccine adverse events risk – short term and long whatever those horrors turn out to be. This chart is all you really need to understand and get to the core informed consent per the Phase III trials and subsequent updates because these researchers have avoided Outcome Reporting Bias.
This is in contrast to what the CDC elected to do on May 1 of this year:
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough cases to focus on identifying and investigating only hospitalized or fatal cases due to any cause. This shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance.
Previous data on all vaccine breakthrough cases reported to CDC from January–April 2021 are available.
That “shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance” is a glaring example of Outcome Reporting Bias. CDC Director Rochelle Walensky’s non-scientific definition of “quality” is in changing accurate counts of infections and the important signal of infection rate (the R0 number) - shifting the well understood goalposts to help confirm a biased outcome. This change in data collection has added a layer of confusion that emerged when the CDC reported on breakthrough cases in an outbreak of 469 people during the July 4 holiday week in Barnstable County, MA in a slide presentation by investigators and found that 74% of the infections were fully vaccinated. That number in Provincetown was 882 infections as of July 29 and the 74% vaccinated rate still holds. Following this inconvenient data, Walensky had to reverse recommendations on mask wearing for the vaccinated, admit the vaccinated can transmit SARSCov2 on par with the unvaccinated and then claim that the infection rate (R0) for the Delta variant sequenced from samples was anywhere from 5 - 9, right up there with chickenpox (see slide 15 chart). This is an explosive rate and quite a change. The revelations that this data provided the CDC was based on an accurate count, not a “quality” control measure over vaccinated infection rates and directly impacted policy and the response to the new surge of Delta variant in the US. When you avoid Outcome Reporting Bias you find yourself actually doing “the Science” however late to the lab.

The First Casualty of War
From the beginning of the blockbuster reports of the Pfizer breakthrough and roll-out is was right there that the genomic vaccine had very little actual promise in both ending the pandemic and mitigating risk for most everyone except the oldest and most vulnerable demographic. It was embedded clearly in the Phase III data itself only the emperor’s “novel” clothes were too dazzling for a nation desperate for some hope out of this pandemic and the lucrative possibilities too tempting for “the Science” to point out the naked truth. Now as we turn another corner and our “independence from this virus” is made an edict that quickly melts like an ice cream cone in the July sun, other spoilers are to blame for this in the corporate media propaganda, inside the White House and CDC. Whether it be the Delta variant or asymptomatic school children or teenagers killing off grandparents, millennials and now most prominently... the unvaccinated, anti-vaxxers and “deplorables”, the goal posts predictably shift once again to explain away how the miracle genomics quickly failed their multi-billion dollar task and the world. I fear we are about to double down, even triple down on them for how deeply invested we are politically, monetarily and emotionally to believe they can save the world. They cannot even prevent infection apparently according to the latest at the CDC– one of the key talking points in the Pfizer NEJM trial abstract discussing the urgent need for a prophylactic to the SARSCov2 virus:
“Safe and effective prophylactic vaccines are urgently needed to contain the pandemic, which has had devastating medical, economic, and social consequences.”
The decision to take them is still technically up to the individual despite a social/genomics engineering apparatus in full throttle to make daily life impossible for informed refuseniks. Once the official approval by the FDA for the vaccine is signed in a couple of weeks – and it will be no doubt – the push to legally mandate in all industries, local governments, businesses, unions and civic affairs will be sealed. And still the pandemic will rage because, in the end, The. Shit. Don’t. Work. At least not in stopping transmission and hardly works but for 1/119 persons in mitigating a moderate infection for the original “wild” SARSCov2. But as the Nuremberg Code is devised to prevent, it will be an ethical, moral and medical catastrophe as this program steamrolls over Informed Consent.
The Illusion of Vaccine Efficacy by Norman Fenton: A brilliant piece on substack with an easy video on youtube is a must read to understand the sham of the “95% efficacy” claim. A placebo can be easily shown to have 95% efficacy under the way the vaccinated are classified and unvaccinated the first 2 or 3 weeks. They rob Peter to pay Paul then they compare the both.
Thanks for this article. I learned a lot. I am now informed about the new bio-tech genomic vaccines like mRNA and that they are very different from traditional vaccines. A very important distinction indeed.
Forgot to mention selling the "product" (vaccines/ weapons) on a global scale to protect against threats they create and exasperate thru the very use of these "products".